


When Reality Feels Unreal
posted 20th March 2026
When Reality Feels Unreal: Understanding Depersonalisation-Derealisation Disorder (DPDR)
In a world where conversations about anxiety and depression are becoming more open, some mental health conditions remain largely misunderstood—even within clinical spaces. One such condition is Depersonalisation-Derealisation Disorder (DPDR), a dissociative disorder that can leave individuals feeling profoundly disconnected from themselves and the world around them. Despite its relatively low profile, it is far from rare and offers an important lens into how the mind copes with overwhelming stress.
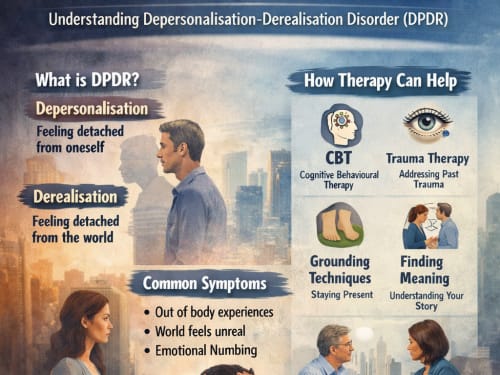
What is DPDR?
Depersonalisation-Derealisation Disorder is characterised by persistent or recurrent experiences of detachment:
Depersonalisation: feeling detached from oneself (e.g., “I feel like I’m watching myself from outside my body”)
Derealisation: feeling detached from the environment (e.g., “the world feels unreal, like a dream or film”)
Individuals typically retain insight, meaning they know these experiences are not literally true—this distinguishes DPDR from psychotic disorders.
Within the DSM-5, DPDR is classified under Dissociative Disorders, reflecting its core feature: a disruption in the integration of consciousness, identity, and perception.
How common is it?
Although often described as “rare” in public discourse, DPDR is estimated to affect around 1–2% of the general population —making it comparable in prevalence to several better-known psychiatric conditions.
More broadly, mental health difficulties are widespread. In England, approximately 1 in 4 people experience a mental health problem each year . This context matters: DPDR does not exist in isolation, but often alongside anxiety, trauma, or depression.
Why does it happen?
From a clinical psychology perspective, DPDR is best understood as a defensive adaptation.
When emotional arousal becomes overwhelming—such as during trauma, panic, or chronic stress—the brain may “dial down” emotional processing. This results in:
- Emotional numbing
- Perceptual detachment
- A sense of unreality
In essence, the mind attempts to protect itself by creating psychological distance.
Recent research trends emphasise that mental disorders are increasingly viewed not as rigid categories but as spectrums of distress, with overlapping symptoms and shared mechanisms . DPDR sits on this spectrum, often co-occurring with anxiety disorders or PTSD.
The lived experience: why it’s so distressing
While DPDR may sound abstract, its impact is deeply unsettling. Clients often report:
Feeling “trapped in their own mind”
Fear of “going crazy”
Loss of emotional connection to loved ones
Hyper-awareness of their own thoughts and perceptions
Paradoxically, it is the awareness of the abnormal experience that fuels anxiety—creating a vicious cycle:
Detachment → anxiety → increased monitoring → intensified detachment
Without intervention, this loop can become chronic.
Where therapy becomes transformative
There is a common misconception that because DPDR involves altered perception, it is somehow less treatable. In reality, psychological therapy is one of the most effective interventions.
The NHS emphasises that evidence-based psychological therapies are central to improving outcomes across severe mental health conditions —and DPDR is no exception.
1. Cognitive Behavioural Therapy (CBT)
CBT helps individuals:
Reframe catastrophic interpretations (“I’m losing my mind”)
Reduce hypervigilance to symptoms
Break the anxiety–dissociation cycle
Over time, this reduces both the frequency and intensity of dissociative episodes.
2. Trauma-focused approaches
Given the strong link with trauma, therapies such as:
EMDR (Eye Movement Desensitisation and Reprocessing)
Trauma-focused CBT
can address underlying emotional overload that drives dissociation.
3. Grounding and embodiment techniques
Clients are taught to reconnect with the present moment through:
Sensory grounding (touch, temperature, sound)
Breathwork
Movement-based awareness
These interventions directly counteract the “disconnection” mechanism at the core of DPDR.
4. A relational, formulation-driven approach
Perhaps most importantly, therapy offers something diagnostic manuals cannot: meaning.
While the DSM-5 provides a shared clinical language, it is ultimately a classification tool rather than a full explanation of lived experience . Therapy moves beyond labels to explore:
Why now?
What function is this serving?
What emotional experiences are being avoided or overwhelmed?
This shift—from symptom to story—is often where recovery begins.
A hopeful prognosis
Unlike some psychiatric conditions, DPDR has a generally positive prognosis with appropriate treatment . Many individuals experience significant improvement or full remission.
The key barriers are not lack of treatment—but:
- Misdiagnosis
- Lack of awareness
- Fear of stigma
- Final reflections
Depersonalisation-Derealisation Disorder challenges our assumptions about what it means to feel “real.” It reminds us that mental health is not simply about mood—but about our fundamental experience of self and reality.
Raising awareness of conditions like DPDR is essential—not only to reduce stigma, but to ensure individuals recognise that what they are experiencing is understandable, treatable, and not a sign of losing control.
Therapy, in this context, is not just symptom reduction. It is the process of reconnecting—gradually and safely—with oneself, others, and the world.