


When OCD and Psychosis Overlap
posted 7th April 2026
Click to enlarge
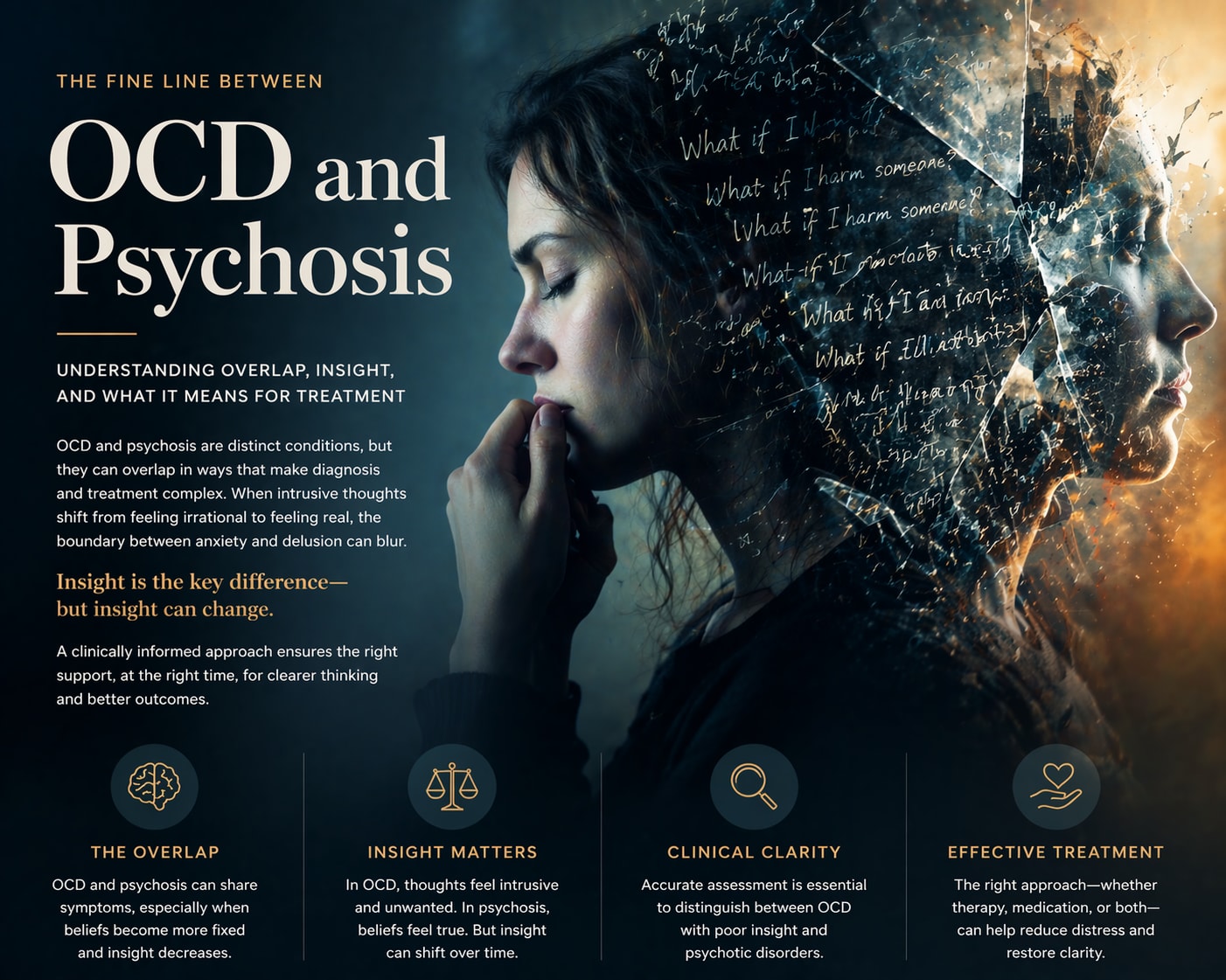
When OCD and Psychosis Overlap: A Clinical Perspective on Intrusive Thoughts and Loss of Insight
Obsessive-Compulsive Disorder (OCD) is typically characterised by intrusive, unwanted thoughts (obsessions) and repetitive behaviours or mental acts (compulsions) aimed at reducing anxiety. In most cases, individuals with OCD recognise that their thoughts are irrational or excessive, even if they feel compelled to act on them. This capacity for insight has traditionally been viewed as a key feature distinguishing OCD from psychotic disorders.
However, in clinical practice, this distinction is not always clear-cut. There are cases in which OCD can begin to resemble psychosis, particularly when insight becomes impaired. Understanding this overlap is essential, both for accurate diagnosis and for ensuring that individuals receive appropriate, effective treatment.
Research suggests that OCD exists on a spectrum of insight. While many individuals retain good insight, others experience what is termed “poor insight” or even “absent insight/delusional beliefs.” In these cases, obsessive thoughts may no longer be recognised as irrational, and instead may be experienced as true or justified. For example, a person who initially recognises that their fear of contamination is excessive may, over time, come to believe that they are genuinely at risk in a way that others cannot understand.
This shift in belief can make OCD appear similar to psychosis, where delusions—fixed, false beliefs—are a defining feature. However, the underlying mechanisms may differ. In OCD, thoughts often remain repetitive, anxiety-driven, and linked to attempts to neutralise distress through compulsions. In contrast, psychotic beliefs are typically more fixed, less responsive to doubt, and not necessarily accompanied by ritualistic behaviours.
The concept of a “schizo-obsessive” spectrum has emerged in the research literature to describe individuals who present with both obsessive-compulsive symptoms and features of psychosis. Studies suggest that a significant minority of individuals with schizophrenia also experience obsessive-compulsive symptoms, and conversely, a smaller subset of individuals with OCD may develop psychotic features. This overlap can complicate both assessment and treatment.
Neurobiological research provides some support for this continuum. Both OCD and psychotic disorders have been associated with dysfunction in fronto-striatal circuits, although the patterns and severity may differ. Additionally, both conditions involve disruptions in how thoughts are evaluated and interpreted, particularly in relation to threat and significance.
A key clinical distinction lies in how thoughts are experienced. In OCD, intrusive thoughts are typically ego-dystonic—they are experienced as inconsistent with the individual’s values and sense of self. Even when insight is reduced, there is often a residual sense of discomfort or internal conflict. In psychosis, by contrast, beliefs are more likely to be ego-syntonic and integrated into the individual’s worldview.
That said, the boundary can become blurred. Under conditions of high stress, sleep deprivation, or severe anxiety, individuals with OCD may experience transient reductions in insight, making their beliefs feel more convincing and less open to challenge. In some cases, this can escalate into what appears to be delusional conviction, particularly if compulsions and avoidance behaviours reinforce the belief over time.
It is also important to recognise that not all unusual or strongly held beliefs indicate psychosis. OCD can involve highly distressing and taboo intrusive thoughts—such as fears of harming others or acting immorally—that are misinterpreted as meaningful or dangerous. Without careful assessment, these experiences can be misunderstood, leading to inappropriate treatment approaches.
From a treatment perspective, distinguishing between OCD with poor insight and psychosis is critical. Evidence-based treatments for OCD, such as Exposure and Response Prevention (ERP), rely on the individual’s ability to question and test their beliefs. When insight is significantly impaired, adaptations may be required, and in some cases, pharmacological interventions typically used in psychosis may be considered.
A balanced clinical approach is therefore essential. Rather than viewing OCD and psychosis as entirely separate categories, it is often more helpful to consider them along a continuum of belief conviction and insight. This allows for a more nuanced understanding of the individual’s experience and supports the development of a tailored treatment plan.
Ultimately, while the overlap between OCD and psychosis can be complex, it is also manageable with appropriate psychological and psychiatric care. With careful assessment and evidence-based intervention, individuals can regain clarity, reduce distress, and re-establish a sense of control over their thoughts and experiences.