


Body Dysmorphic Disorder in the Age of Social Media
posted 17th April 2026
Body Dysmorphic Disorder in the Age of Social Media: Clinical Understanding and Evidence-Based Treatment
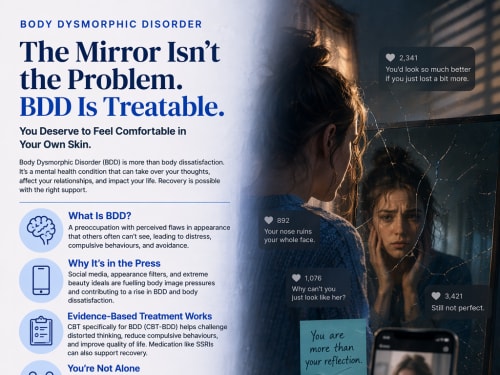
Body Dysmorphic Disorder (BDD) is an increasingly visible mental health condition, receiving growing attention in both clinical settings and public discourse. Characterised by a preoccupation with perceived flaws in appearance—often unnoticeable to others—BDD can lead to significant distress, functional impairment, and compulsive behaviours such as mirror checking, excessive grooming, or seeking cosmetic procedures. While BDD has long been recognised within psychiatric literature, recent cultural and technological shifts—particularly the rise of social media and appearance-focused platforms—have intensified its relevance in contemporary clinical practice.
Recent media coverage has highlighted the resurgence of extreme body ideals and the influence of “skinny” and aesthetic-driven online trends, which may exacerbate body dissatisfaction and contribute to disordered thinking about appearance . Alongside this, the rapid growth of weight-loss medications and digitally mediated self-image has raised concerns among clinicians about the psychological consequences of appearance-focused behaviours, including the development or worsening of body image disturbances . These sociocultural dynamics provide an important backdrop for understanding the increasing presentation of BDD in clinical settings.
From a psychological perspective, BDD is conceptualised within a cognitive-behavioural framework. Individuals with BDD tend to develop maladaptive beliefs about the importance of appearance, often equating self-worth with physical attractiveness. These beliefs are maintained through attentional biases (e.g., selective focus on perceived flaws), cognitive distortions (e.g., catastrophising minor imperfections), and safety behaviours (e.g., avoidance of social situations, reassurance seeking). Neurobiological research further suggests abnormalities in visual processing and emotional regulation, with individuals showing heightened sensitivity to detail and threat-related stimuli.
BDD frequently co-occurs with other mental health conditions, including depression, social anxiety, and obsessive-compulsive disorder (OCD). This comorbidity profile reinforces its classification within the obsessive-compulsive and related disorders spectrum in the DSM-5. Importantly, individuals with BDD are at significantly elevated risk of suicidality, underlining the seriousness of the condition and the need for early identification and intervention.
In terms of treatment, Cognitive Behavioural Therapy specifically adapted for BDD (CBT-BDD) remains the first-line psychological intervention. This approach focuses on challenging distorted beliefs about appearance, reducing compulsive behaviours, and addressing avoidance patterns. Techniques such as cognitive restructuring, exposure and response prevention (ERP), and perceptual retraining are central components of treatment. A substantial body of research supports the efficacy of CBT in reducing symptom severity and improving functional outcomes, particularly when delivered by clinicians with specialist expertise.
Pharmacological interventions, particularly selective serotonin reuptake inhibitors (SSRIs), are also recommended, especially in moderate to severe cases. SSRIs have been shown to reduce obsessive preoccupations and compulsive behaviours, although they are typically used in conjunction with psychological therapy rather than as standalone treatments. As with eating disorders, medication is often most effective when embedded within a broader, multidisciplinary treatment plan.
A critical challenge in treating BDD lies in help-seeking behaviour. Many individuals do not initially present to mental health services, instead seeking cosmetic or dermatological interventions. However, research consistently demonstrates that cosmetic procedures rarely alleviate BDD symptoms and may, in some cases, exacerbate psychological distress. This highlights the importance of screening for BDD in aesthetic and medical settings, as well as increasing public awareness of the condition.
Early intervention is particularly important. Given the developmental trajectory of BDD—often emerging in adolescence—timely identification can significantly improve long-term outcomes. Psychoeducation, family involvement, and addressing comorbid difficulties are all key components of effective treatment planning. In clinical practice, establishing a strong therapeutic alliance is essential, as individuals with BDD may experience shame, secrecy, or ambivalence about treatment.
In conclusion, Body Dysmorphic Disorder represents a significant and growing clinical concern, particularly within a cultural context that increasingly emphasises appearance and self-presentation. The convergence of social media, digital self-image, and emerging weight-loss trends has amplified risk factors associated with body dissatisfaction and distorted self-perception. Evidence-based treatment—primarily CBT-BDD supported by pharmacotherapy where appropriate—offers a robust framework for recovery. For psychology clinics, the priority lies in early detection, specialist intervention, and delivering compassionate, individualised care that addresses both the cognitive and emotional dimensions of the disorder.
Click to enlarge